GLP-1 Pill vs. Injection: Which Weight Loss Option is Right for You?

Medical Disclaimer: The information provided in this article is for educational and informational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult with a qualified healthcare provider before making any changes to your medication or weight management plan.
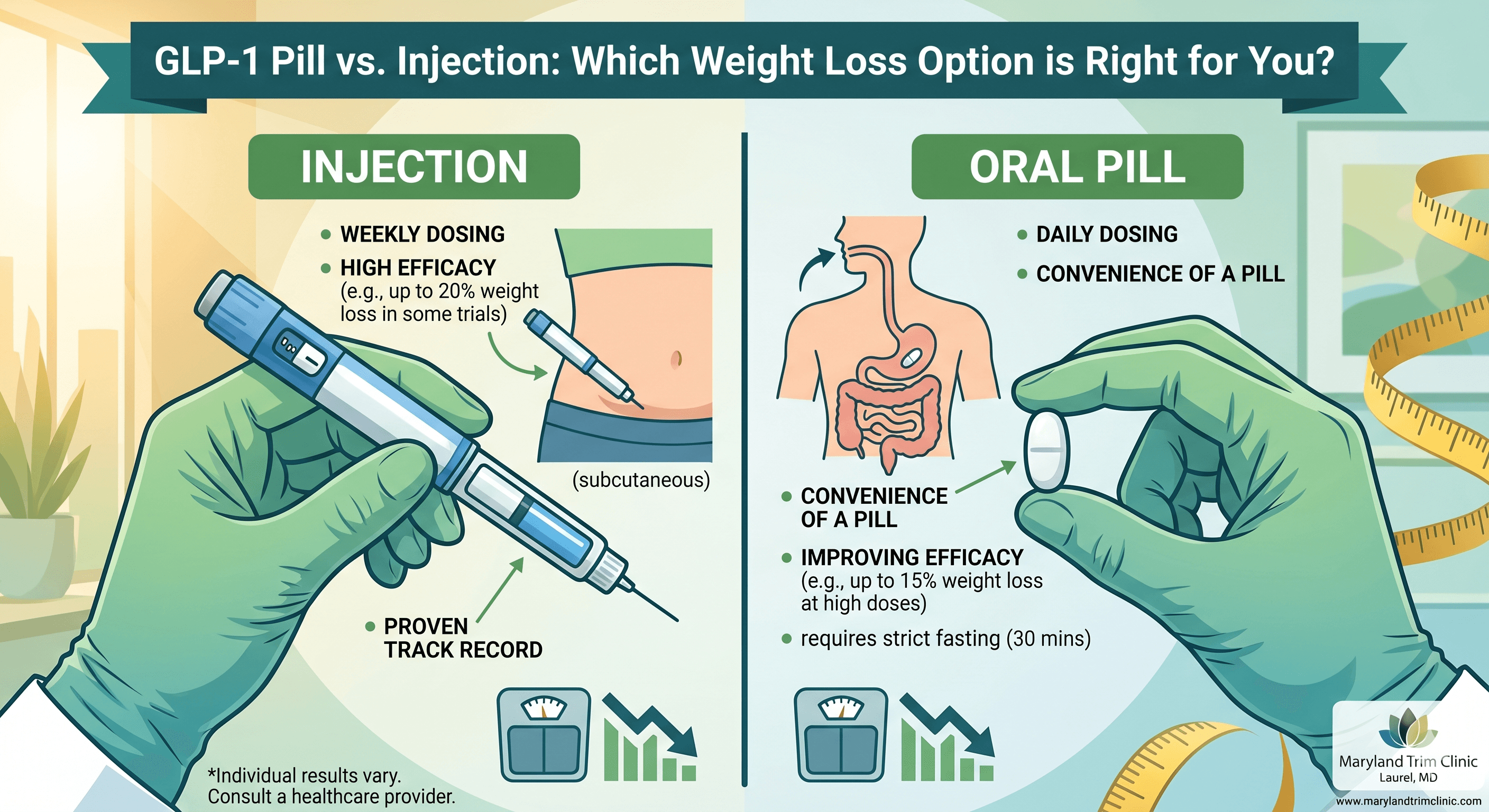
The pill is more convenient — but is it as effective as the shot?
That single question is now sitting at the center of one of the most consequential treatment decisions in modern metabolic medicine. GLP-1 receptor agonists — once confined to injectable pens — have crossed into tablet form, giving patients a new option that feels less clinical and more approachable.
But convenience and clinical effectiveness are not always the same thing. Patients and doctors face a real decision between injectable and oral GLP-1s, with trade-offs that remain genuinely unclear to many who are weighing their options. Whether you are exploring options with your primary care provider or seeking guidance from specialized clinics like Maryland Trim Clinic, understanding the science is the first step.
This article breaks down the evidence side by side: what the data actually shows about weight loss, how adherence patterns differ between the two formats, and what biological risks emerge specifically when GLP-1 therapy is delivered through the digestive tract rather than directly into tissue.
Efficacy Face-Off — What Cross-Trial Data Reveals About Weight Loss Outcomes
Let's start with the metric most patients prioritize: how much weight can you expect to lose?
The Injectable Benchmark
The injectable GLP-1s currently dominate this conversation for a straightforward reason — the trial data is more mature, the doses are higher, and the results are more dramatic. GLP-1 weight loss injections delivered subcutaneously have established a high bar in modern treatment.
- Semaglutide (Ozempic/Wegovy): Delivered as a weekly injection, this has been the benchmark since the STEP trial program published results showing average weight loss of approximately 14.9% of body weight over 68 weeks at the 2.4 mg dose.
- Tirzepatide (Mounjaro/Zepbound): Targeting both GLP-1 and GIP receptors, the SURMOUNT-1 trial reported average weight loss of up to 20.9% at the highest dose.
These are landmark figures in a field that historically struggled to move the needle beyond 5–8% with lifestyle interventions alone, a shift heavily documented in clinical reviews by the National Institutes of Health (NIH).
The Oral Contender
Oral semaglutide — branded as Rybelsus for type 2 diabetes and under active investigation at higher doses for obesity — tells a different story. The OASIS 1 trial, which used a 50 mg daily oral semaglutide dose, reported average weight loss of approximately 15.1% of body weight over 68 weeks in adults with obesity.
On the surface, that number looks highly competitive. However, cross-trial comparisons demand caution. These studies used different patient populations, different inclusion criteria, and different background lifestyle intervention protocols. No head-to-head randomized controlled trial between oral and injectable semaglutide at obesity-indicated doses has been published at the time of this writing.
The Absorption Challenge
What the indirect data does suggest is that the efficacy gap is narrowing, particularly as oral dose escalation protocols mature. Earlier oral semaglutide formulations (3 mg, 7 mg, 14 mg) produced far more modest weight reductions in the range of 2–5%. The jump to 50 mg changes that calculus meaningfully.
Still, the absolute bioavailability of oral semaglutide remains low. It is estimated at roughly 1% compared to the near-complete absorption of injected formulations. This pharmacokinetic reality explains why the oral dose must be so much higher to achieve comparable plasma levels, which has downstream implications for both safety and efficacy.
Bottom line on efficacy: Injectables currently hold the proven edge in average weight loss outcomes based on available trial data. Oral semaglutide at 50 mg is a genuine contender, but not yet a proven equal. Patients with the most aggressive weight loss goals should have a frank conversation with their provider about these differences.
Convenience & Adherence — Why the Daily Pill May Win the Long Game
Efficacy data from clinical trials captures what a drug can do under controlled conditions. Adherence data captures what patients actually do in the real world — and that distinction matters enormously for chronic disease management.
The Friction of the Needle
Needle aversion is not a minor inconvenience; it is a profound barrier to care. For patients who delay starting an injectable GLP-1 — or who quietly discontinue it after a few doses — the theoretical efficacy advantage of the shot becomes irrelevant. A pill that gets taken consistently will always outperform an injection that sits unused in the refrigerator.
Beyond needle aversion, the logistics of injectable therapy carry their own friction:
- Auto-injector pens require refrigeration until first use.
- They demand proper sharps disposal.
- The routine can be difficult to maintain through travel, shift work, or disrupted schedules.
The Psychology of the Pill
A daily oral tablet, by contrast, integrates more naturally into existing morning routines. For many patients, swallowing a pill feels less like a medical intervention and more like standard self-care. This perceived normalcy may reduce the stigma some patients associate with obesity treatment and lower the psychological barrier to long-term continuation.
The Oral Fasting Protocol: A New Type of Hurdle
That said, the oral GLP-1 is not without its own strict adherence demands. Oral semaglutide must be taken under very specific conditions:
- Empty Stomach: Must be taken immediately upon waking.
- Minimal Liquid: Taken with no more than 4 oz (120 mL) of plain water.
- The Waiting Game: You must wait at least 30 minutes before eating, drinking anything else, or taking other daily medications.
This strict fasting window is not a mere suggestion — it is pharmacologically necessary. Semaglutide’s already-low oral bioavailability is further compromised by food, fluids, or other drugs. Patients who cannot reliably meet these conditions may find the oral format surprisingly burdensome, effectively trading one type of adherence challenge for another.
The Verdict — Biological Risks Unique to Oral Delivery
Convenience and efficacy are the two factors patients most often ask about. But there is a third axis that deserves equal weight in the clinical conversation: the biological risks that emerge specifically because of how the oral formulation is engineered to work.
Human digestive system - Gastric mucosa and Layers of the Stomach.
The Role of SNAC
To survive the harsh environment of the gastrointestinal tract, oral semaglutide is co-formulated with an absorption enhancer called SNAC (sodium N-[8-(2-hydroxybenzoyl) amino] caprylate).
- How it works: SNAC transiently raises the local pH in the stomach and facilitates the absorption of semaglutide directly through the stomach lining (gastric mucosa).
- The concern: While this mechanism is clever, SNAC involves direct contact with and mild perturbation of the gastric lining.
Gastric Health Considerations
While short-term trial data has not revealed alarming signals of mucosal injury at currently approved doses, the long-term effects of daily SNAC exposure at higher doses remain an active area of inquiry. Patients with pre-existing gastric conditions — including gastritis, peptic ulcer disease, or a history of gastric surgery — warrant individualized assessment before initiating oral semaglutide.
Interactions and Side Effects
Drug-drug interactions represent another underappreciated risk. Because oral semaglutide requires a 30-minute exclusive window, patients taking multiple morning medications (like thyroid hormones or blood pressure pills) face real scheduling complexity.
Furthermore, while gastrointestinal side effects (nausea, vomiting) are common to all GLP-1 therapies, the oral route may concentrate upper GI effects uniquely. Taking a potent medication on an empty stomach can amplify nausea in sensitive individuals.
The Verdict: Neither format is risk-free. Injectable GLP-1s carry their own well-documented concern profile, monitored closely by regulatory bodies like the U.S. Food and Drug Administration (FDA), including potential gallbladder disease and pancreatitis signals. However, oral delivery introduces a distinct, localized set of risks centered on the stomach environment that must be weighed carefully.
Bringing It Together: A Framework for the Decision
For most patients, the decision is not purely scientific — it is personal.
To help frame your conversation with your doctor or when exploring metabolic testing and analysis to personalize your care, consider this quick-reference guide:
Consider the Injectable Format If:
- You want the highest statistically proven potential for overall weight loss.
- You prefer a "once-a-week" routine over a daily medication burden.
- You take multiple morning medications that cannot be delayed.
- You have a history of sensitive stomach issues, gastritis, or stomach ulcers.
Consider the Oral Format If:
- You have significant anxiety or aversion to needles and self-injections.
- You already have a reliable morning routine and take daily pills.
- You frequently travel and find refrigerating/transporting injectable pens cumbersome.
- You are fully capable of committing to the strict 30-minute morning fasting window.
What is not acceptable is treating this as a trivial choice. Patients deserve full transparency regarding efficacy, convenience, and safety before they decide which format fits their life.
Maryland Trim Clinic (MTC) in Laurel, MD
Navigating the complexities of GLP-1 medications—whether oral or injectable—requires expert, personalized guidance rather than a one-size-fits-all prescription. Located in Laurel, MD, Maryland Trim Clinic (MTC) provides a supportive, medically supervised environment for patients seeking sustainable metabolic health.
Instead of leaving patients to figure out dosing schedules and side effect management on their own, a comprehensive medical weight loss program like the one at MTC ensures that your treatment aligns with your unique biological needs, lifestyle, and medical history. Whether you need support managing the oral fasting protocol, overcoming needle anxiety, or tracking your long-term progress, working closely with dedicated clinical professionals can make the difference between a frustrating trial and a successful health transformation.
Frequently Asked Questions
Q: Is oral semaglutide as effective as injectable semaglutide for weight loss?
A: Based on current trial data, oral semaglutide at 50 mg shows weight loss results that approach those of injectable semaglutide at 2.4 mg (approximately 15% body weight reduction). However, no direct head-to-head randomized trial has been completed, and injectable medications like tirzepatide still lead the field. The pill is competitive, but injectables currently hold the edge for aggressive weight loss.
Q: Why does oral semaglutide require such a high dose compared to the injection?
A: Oral semaglutide has an estimated bioavailability of only about 1%, meaning the vast majority of the drug is degraded in the stomach. The 50 mg oral dose is engineered to be high enough that even this small fraction of absorption delivers meaningful blood levels. Injections bypass the digestive tract entirely, achieving near-complete absorption at much lower doses.
Q: What is SNAC and why does it matter for safety?
A: SNAC is an absorption enhancer co-formulated with the GLP-1 pill to help it survive the stomach and enter the bloodstream. It alters the gastric environment to push the drug through the stomach lining. Patients with pre-existing stomach conditions (like ulcers) should discuss this specifically with their provider.
Q: Can I take my other morning medications at the same time as oral semaglutide?
A: No. You must take the pill on an empty stomach with a small sip of plain water, then wait at least 30 minutes before eating, drinking, or taking any other medications. Food and other substances significantly block the drug's absorption.
Q: Are the side effects different between the pill and the injection?
A: Both formats share classic side effects: nausea, vomiting, diarrhea, constipation, and reduced appetite. However, the oral route involves direct stomach exposure, and taking it on an empty stomach can sometimes worsen upper GI discomfort. Injectables bypass the stomach but can cause injection-site reactions.
Ready to Find the Right Approach for Your Body?
Choosing between a GLP-1 pill and an injection is a medical decision that requires professional insight and a deep understanding of your personal metabolic health. Don't navigate it alone. Speak with the experts to build a tailored plan that fits your lifestyle, your goals, and your biology. Reach out to your healthcare provider or a dedicated medical weight loss specialist today to get started on a safer, more effective path to wellness.