Tens of Millions on GLP-1s: The Societal Impact of Weight Loss Meds

Tens of millions of Americans are now utilizing the same weight loss medication — and it is already changing how the world is built around us.
It started quietly. A few years ago, GLP-1 receptor agonists like semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound) were niche medications first developed for Type 2 diabetes. Then came the celebrity endorsements, the viral testimonials, and headline-grabbing clinical trials showing 15–20% body weight reduction.
Almost overnight, appetite suppressant medications moved from specialty clinics into the cultural mainstream. By 2024, estimates suggested that more than 12 million Americans had a GLP-1 prescription—a number analysts project could swell to 30 million by the end of the decade.
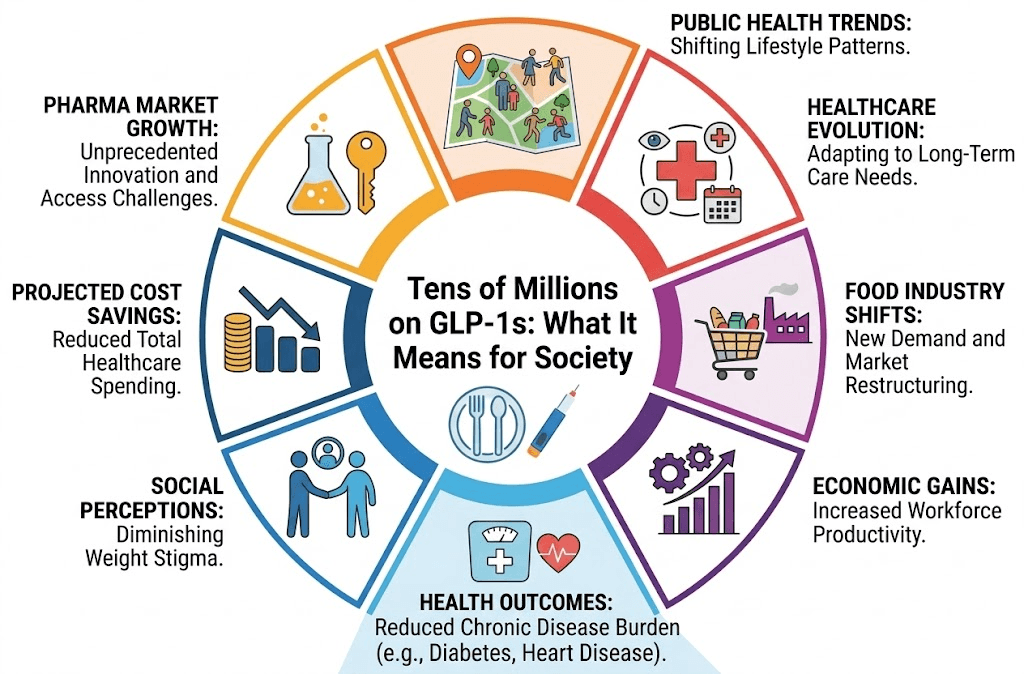
When tens of millions of people change something as fundamental as how their bodies process appetite, the downstream effects are not just medical. They are economic, architectural, psychological, and deeply political. This is the story of what happens when a single class of drugs becomes a societal force—and why the full consequences are only beginning to come into focus.
ACT 1: The Industries Already Feeling the Shift
The food industry noticed first. Consumer packaged goods giants—companies like Nestlé, Conagra, and General Mills—began quietly adjusting their product strategies after data showed that GLP-1 users were eating significantly less and, crucially, eating differently.
GLP-1 medications don't just suppress appetite; they appear to alter brain chemistry to reduce cravings for ultra-processed, high-fat, and high-sugar foods. Users report losing interest in the snack foods and fast food that make up a significant share of the standard American diet.
The Economic Ripple Effects:
- Wall Street Reactions: Shares in major snack food companies dipped as analysts modeled what a GLP-1-saturated market meant for long-term revenue. Conversely, companies selling high-protein, nutrient-dense foods (like Greek yogurt and lean meats) saw increased investor interest.
- Restaurant Adaptations: Several major chains have begun reducing portion sizes. Smaller plates and protein-forward menus are emerging trends explicitly acknowledging that the customer base is physically changing.
- Fashion Industry Shifts: For decades, the $40 billion U.S. plus-size clothing market was a rapidly growing retail segment. Now, some retailers are reporting slowing growth in extended sizes while simultaneously seeing surges in mid-range sizes.
- Urban Planning: Airlines, theme parks, and public transit systems that spent decades expanding seat sizes and weight limits are now watching GLP-1 trends to see if population-level weights will shift infrastructure needs again.
The economic ripple effects are real and measurable. But they are only the surface layer of something far more consequential.
ACT 2: The Public Health Calculus — Promise and Peril
The public health case for widespread GLP-1 adoption is, on its face, compelling. The Centers for Disease Control and Prevention (CDC) notes that obesity is a documented risk factor for Type 2 diabetes, cardiovascular disease, and certain cancers, costing the U.S. healthcare system an estimated $173 billion annually.
If GLP-1 medications can meaningfully reduce population-level obesity rates, the downstream savings in human suffering and medical expenditure could be enormous. The clinical evidence is genuinely exciting: trials have shown that these drugs not only help people lose weight but fundamentally alter chronic disease trajectories, reducing the risk of heart attacks and strokes.
But the picture is not without shadows.
The Unanswered Questions
The Rebound Reality: Studies consistently show that most users regain a significant portion of lost weight within months of discontinuation. For most, these drugs are not a cure; they are a chronic treatment requiring indefinite use. The long-term safety profile of decades-long GLP-1 use is simply not yet known.
Medical Side Effects: While highly effective, these drugs carry risks. Nausea and GI distress are common. More serious concerns include gastroparesis (severely delayed stomach emptying) and muscle mass loss if not paired with proactive muscle building and toning.
The Psychological Dimension: Obesity exists at the intersection of genetics, environment, mental health, and socioeconomic stress. Medicalizing weight loss at this scale could inadvertently reinforce the stigma that heavier bodies are problems to be pharmacologically solved, doing little to address the food environments and systemic inequities that drive obesity in the first place.
Public health is rarely a story with clean heroes and villains. GLP-1s represent a genuine breakthrough in metabolic medicine. They also represent a set of medical and systemic risks that demand serious scrutiny.
ACT 3: The Equity Gap — Who Gets Left Behind
Here is the uncomfortable truth sitting at the center of the GLP-1 moment: the people most likely to benefit from these medications are the least likely to access them.
Obesity rates in the United States are not evenly distributed. Minority and lower-income populations often face higher rates of obesity driven by structural factors—food deserts, economic insecurity, and historical underinvestment in community health. These are precisely the populations for whom GLP-1 medications could have the greatest impact.
The Cost Barrier: Wegovy and Zepbound carry list prices of approximately $1,000 to $1,350 per month. While manufacturer coupon programs exist, they are often inaccessible to people on Medicaid or Medicare. Private insurance coverage is inconsistent, with many employers explicitly excluding GLP-1s for obesity from their formularies due to cost concerns.
The result is a tiered system in which GLP-1 access largely correlates with economic privilege. A 2023 analysis found that GLP-1 users skewed heavily toward higher-income zip codes and commercially insured patients.
If GLP-1s become the defining medical story of the 2020s, their legacy will be written not just by who they helped—but by who they couldn't reach.
Maryland Trim Clinic (MTC) in Laurel, MD
As the medical weight loss landscape continues to shift at a societal level, individual patients need a reliable, evidence-based partner to navigate their own health journey. Located in Laurel, MD, the Maryland Trim Clinic (MTC) provides the structured, medically supervised framework necessary to access these breakthrough therapies safely and effectively.
MTC understands that a prescription alone is not a comprehensive health strategy. For patients utilizing GLP-1 weight loss injections, our clinical team focuses on long-term, holistic wellness. When you enroll in a medical weight loss program, you receive more than just medication. Through metabolic testing and analysis and robust nutritional counseling and coaching, MTC ensures that your body composition improves, your muscle is protected, and your weight loss is sustainable—protecting you against the common pitfalls of the GLP-1 era.
The Bigger Picture
GLP-1 drugs are real, and their potential is real. The clinical evidence for their efficacy in weight reduction and cardiovascular protection is among the most robust seen in metabolic medicine in decades. The industries bending to accommodate a changing American body are doing so rationally.
But history counsels humility when a single intervention is positioned as the answer to a complex societal problem. The National Institutes of Health (NIH) emphasizes that obesity is the product of complex socio-economic, environmental, and biological factors. GLP-1s can work beautifully alongside efforts to address those systems, but they cannot substitute for them.
The tens of millions now on these medications are participating in an unprecedented natural experiment. What we learn from them will shape medicine, policy, and culture for generations. The least we can do is pay close attention, ask hard questions, and insist that the benefits of this moment are shared as broadly as the burdens of obesity have always been.
Medical Disclaimer: The information provided in this article is for educational purposes only and is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician regarding a medical condition, treatment options, or before altering your prescribed medication routine.
Frequently Asked Questions
Q: What are GLP-1 medications and how do they work? A: GLP-1 receptor agonists mimic a naturally occurring hormone released after eating. They suppress appetite, reduce cravings for high-fat and high-sugar foods, and slow the rate at which the stomach empties, leading to significantly reduced caloric intake and weight loss.
Q: How many Americans are currently using GLP-1 drugs for weight loss? A: As of 2024, approximately 12 million Americans held active GLP-1 prescriptions. Analysts project this figure could reach 30 million or more by the end of the decade, driven by expanding access and new FDA approvals.
Q: What happens when people stop taking GLP-1 medications? A: Clinical studies consistently show that the majority of people who discontinue GLP-1 medications regain a substantial portion of the weight they lost—often 50–70% within 12 months. Because the drugs manage the biological signals driving appetite rather than curing them, most users require indefinite treatment to maintain results.
Q: Are there serious side effects associated with GLP-1 medications? A: The most common side effects are gastrointestinal (nausea, diarrhea, constipation). More serious concerns under ongoing medical review include gastroparesis (severely delayed stomach emptying), pancreatitis, and potential muscle mass loss if patients do not intentionally consume high protein and strength train.
Q: Why do GLP-1 drugs cost so much in the United States compared to other countries? A: The United States lacks the centralized drug price negotiation systems used in countries like Germany and Canada. Consequently, list prices for GLP-1 drugs in the U.S. can reach $1,000–$1,350 per month, contributing to a massive equity gap in access.
Q: How is the food industry responding to the rise of GLP-1 medications? A: Major food companies are adjusting product strategies as GLP-1 users eat less and crave fewer ultra-processed foods. Snack sectors have faced investor skepticism, while protein-rich, nutrient-dense food categories have seen increased commercial interest and growth.
Q: What does the equity gap in GLP-1 access actually look like in practice? A: Prescription data shows that GLP-1 users are disproportionately concentrated in higher-income, commercially insured populations. Meanwhile, lower-income Americans—who bear the heaviest burden of obesity-related illnesses—often cannot afford the medications due to lack of comprehensive insurance coverage.
Ready to Navigate Your Medical Weight Loss Journey?
In a rapidly changing medical landscape, you need expert guidance to achieve your health goals safely. Visit the Maryland Trim Clinic homepage today to schedule a consultation. Our clinical team in Laurel, MD, is ready to provide the comprehensive support you need for sustainable success.