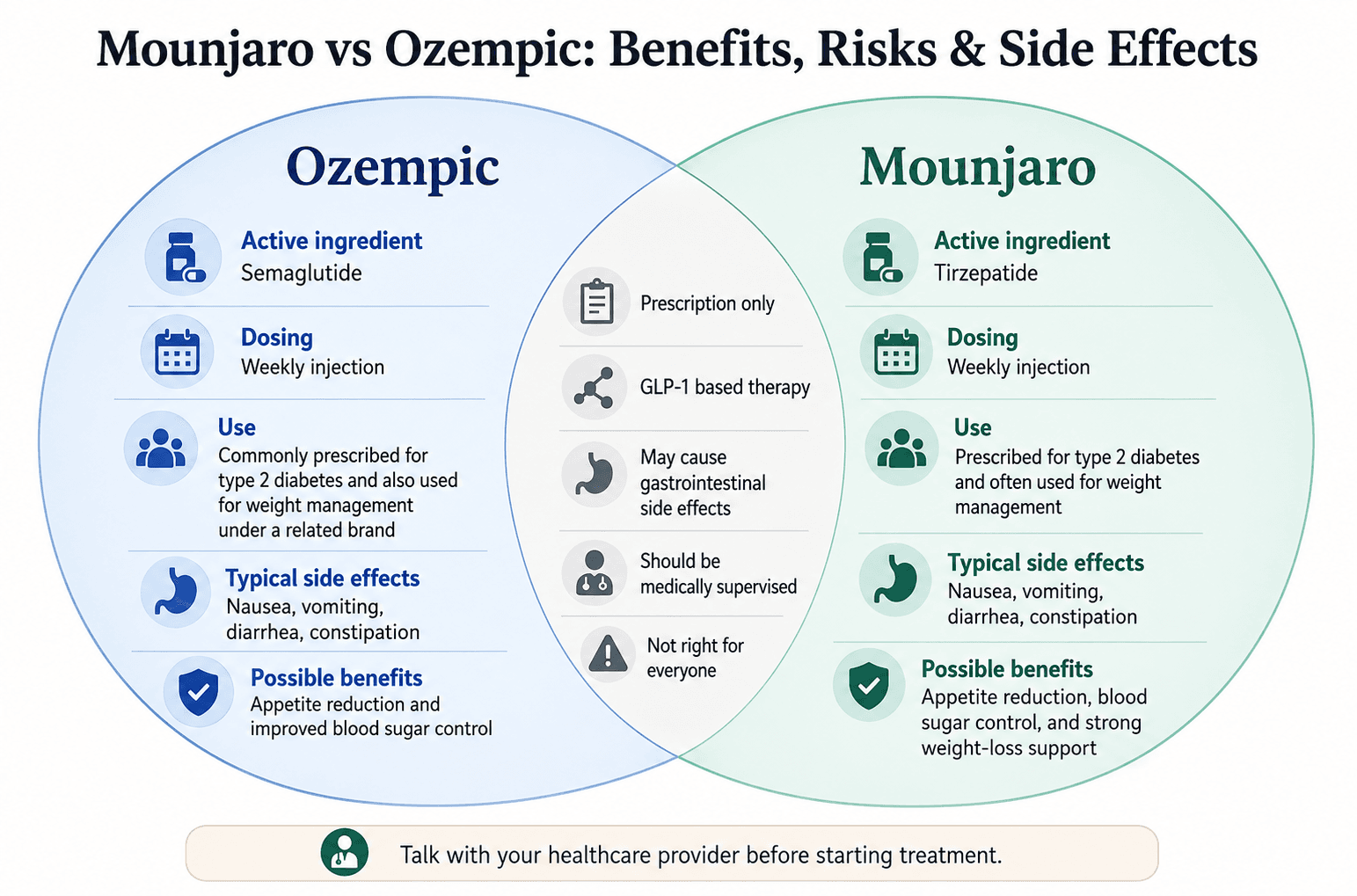
Mounjaro vs Ozempic: Benefits, Risks & Side Effects


Before you inject anything, you need to hear the whole truth about Mounjaro and Ozempic.
Not the version filtered through pharmaceutical marketing. Not the celebrity version where every story sounds effortless. Not the fear-based version that treats every injection like a guaranteed medical disaster.
The real story is more balanced, more biological, and more personal.
Mounjaro and Ozempic belong to a class of medications that can meaningfully change appetite, blood sugar, weight, cravings, and the way some people experience food. For many patients, especially those with type 2 diabetes, obesity, or weight-related health concerns, these medications can be powerful tools when prescribed and monitored appropriately.
But they are not magic. They are not risk-free. They are not a substitute for nutrition, resistance training, medical supervision, or long-term planning. And they are not the right choice for everyone.
If you are considering one of these medications, you deserve a clear explanation of what they actually do, what they may cost you physically and financially, and how to think through the decision without hype or panic.
Let’s start from the beginning.
What These Drugs Actually Do Inside Your Body
First, a quick naming clarification
People often use “Mounjaro” and “Ozempic” as shorthand for weight-loss injections, but the names matter.
Mounjaro is the brand name for tirzepatide used for adults with type 2 diabetes. Tirzepatide is also FDA-approved under the brand name Zepbound for chronic weight management in eligible adults, along with reduced-calorie eating and increased physical activity. The FDA’s announcement on tirzepatide for chronic weight management explains the approved weight-management use.
Ozempic is the brand name for semaglutide used for adults with type 2 diabetes. Semaglutide is also FDA-approved under the brand name Wegovy for chronic weight management in eligible patients. The FDA has also summarized its approval of semaglutide for chronic weight management.
That distinction matters because insurance coverage, dosing, medical criteria, and labeling can differ by brand and indication.
How GLP-1 signaling changes appetite and blood sugar
GLP-1 stands for glucagon-like peptide-1. It is not a pharmaceutical invention. It is a hormone your gut naturally produces, especially after eating.
Under normal conditions, GLP-1 helps your body:
- release insulin when blood sugar rises
- reduce glucagon when appropriate
- slow how quickly food leaves the stomach
- send fullness signals to the brain
- reduce appetite after a meal
GLP-1 medications imitate or amplify this natural pathway, but they last much longer in the body than your natural GLP-1 hormone.
That is why people often feel full sooner, eat smaller portions, and experience fewer cravings. They are not simply “trying harder.” The medication changes the biological signals involved in hunger, fullness, and blood sugar regulation.
For someone who has struggled for years with intense hunger, constant cravings, or blood sugar instability, that can feel dramatic.
Why Mounjaro works differently from Ozempic
Ozempic, or semaglutide, is a GLP-1 receptor agonist. That means it activates GLP-1 receptors involved in appetite, insulin response, and digestion.
Mounjaro, or tirzepatide, activates two related hormone pathways: GLP-1 and GIP. GIP stands for glucose-dependent insulinotropic polypeptide, another gut hormone involved in insulin regulation and metabolic signaling.
This dual action is one reason tirzepatide has generally produced greater average weight loss than semaglutide in several obesity-focused trials. But “greater average weight loss” does not automatically mean “better for everyone.”
The better medication depends on:
- your diagnosis
- your weight and health goals
- your blood sugar status
- your heart and kidney history
- your side effect tolerance
- your contraindications
- your insurance coverage
- your ability to sustain treatment
- your clinician’s judgment
The goal is not to choose the most aggressive option. The goal is to choose the most appropriate and sustainable option for your body.
What “food noise” really means
One of the most common phrases people use with these medications is “food noise.”
Food noise is the persistent mental chatter about food: what to eat, when to eat, whether there is food nearby, whether you should snack, whether you can resist a craving, whether you already “ruined” the day.
For some people, GLP-1 medications dramatically reduce that background noise.
That can feel like freedom. Meals become less emotionally charged. Cravings may feel less urgent. Portions may become easier to control. Some people describe being able to make food decisions without feeling like they are fighting themselves all day.
This is not just willpower. These medications act on appetite and reward pathways in the brain as well as digestive and metabolic pathways in the body.
But that also explains why the experience can feel emotionally complicated. Food is not only fuel. It can be comfort, culture, routine, celebration, stress relief, and social connection. When the medication changes appetite and reward signals, it may also change your relationship with food.
What these medications do not do
Mounjaro and Ozempic do not replace the basics of long-term health.
They do not automatically preserve muscle. They do not teach you how to eat enough protein. They do not fix poor sleep, emotional eating, stress patterns, or inactivity by themselves. They do not remove the need for medical monitoring.
They create a biological window of opportunity.
What you do inside that window still matters.
A responsible plan should include:
- medical supervision
- realistic goal-setting
- nutrition planning
- adequate protein
- resistance training or strength-focused movement
- hydration
- side-effect monitoring
- long-term maintenance planning
- emotional and behavioral support when needed
Without that structure, people may lose weight but feel weak, undernourished, anxious about stopping, or unprepared for maintenance.
The Risks Nobody Puts in the Brochure
Here is where the conversation needs to be more honest.
The risks are not a reason to panic. They are a reason to be informed.
Many people tolerate these medications well. Others deal with side effects that meaningfully affect daily life. Some side effects are uncomfortable but manageable. Others require prompt medical attention.
The safest position is neither “these drugs are miracles” nor “these drugs are dangerous for everyone.”
The safest position is: these are powerful prescription medications that should be used carefully, monitored properly, and understood clearly.
Gastrointestinal side effects can be more than “mild discomfort”
Nausea, vomiting, diarrhea, constipation, reflux, burping, bloating, and stomach discomfort are among the most common complaints.
That makes sense because these medications slow gastric emptying and change appetite signaling. Food may stay in the stomach longer. Large meals may feel heavier. Greasy foods may become harder to tolerate. Alcohol may hit differently. Skipping meals may trigger nausea instead of preventing it.
Some people adjust within a few weeks. Others struggle each time the dose increases.
A practical way to manage the early GI phase:
- If you feel nauseated: eat smaller meals, sip fluids, avoid greasy foods, and ask your clinician about options if nausea disrupts your life.
- If you feel constipated: increase fluids, add fiber gradually, walk when possible, and ask before using laxatives or supplements.
- If you have diarrhea: simplify meals, replace fluids, avoid trigger foods, and call your clinician if symptoms are severe or persistent.
- If reflux worsens: avoid lying down after meals, reduce late-night eating, and discuss persistent symptoms with your healthcare provider.
- If you cannot keep fluids down: do not wait too long before seeking medical guidance.
Mayo Clinic’s overview of tirzepatide precautions and side effects is a helpful reminder that side effects should be monitored, especially when symptoms are severe, persistent, or unusual.
Muscle loss deserves more attention
Weight loss is not automatically the same as fat loss.
When people lose weight quickly, they may lose a mix of fat, water, and lean mass. Lean mass includes muscle, and muscle matters for strength, metabolism, balance, aging, and daily function.
This is one of the most under-discussed issues with GLP-1 and GIP-based medications.
Because appetite can drop so sharply, some people unintentionally under-eat. They may skip meals, avoid protein because they feel too full, or rely on very small portions that do not support muscle maintenance.
The result can be frustrating: the scale goes down, but energy drops, strength decreases, and the body feels less firm or less capable.
To reduce that risk, focus on:
- protein at each meal
- resistance training 2 to 3 times weekly, if medically appropriate
- gradual progression rather than extreme workouts
- enough calories to support basic function
- hydration and sleep
- body measurements and strength markers, not only scale weight
This is where structured support can make a difference. Some patients benefit from nutrition counseling and coaching to help them eat enough while still supporting weight-management goals. Others may use 3D body scanning to track changes beyond the number on the scale.
Regain after stopping is a real possibility
This is one of the hardest truths.
Many people regain weight after stopping GLP-1 medications, especially if the medication was doing most of the appetite regulation and long-term habits were not fully established.
That does not mean the medication “failed.” It means obesity and weight regulation are biological, chronic, and complex for many people.
These medications work while they are active in the body. When they are stopped, appetite signals may return. Food noise may increase. Portions may become harder to manage. The body may push back toward a previous weight range.
Before starting, it is wise to ask:
- Can I sustain this medication if it works?
- What happens if insurance stops covering it?
- What is my plan if I need to stop?
- Am I building habits while appetite is quieter?
- How will I monitor regain without panic?
- What support will I need for maintenance?
This is why medication should be framed as one part of a long-term plan, not a short-term shortcut.
Pancreatitis, gallbladder issues, and thyroid warnings
Serious side effects are uncommon, but they matter.
Both semaglutide and tirzepatide labels include warnings that patients should understand before treatment. These include risks related to pancreatitis, gallbladder problems, low blood sugar when combined with certain diabetes medications, kidney problems related to dehydration, and a boxed warning about thyroid C-cell tumors based on animal studies.
The thyroid warning is especially important for people with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2. These medications are generally not used in those situations.
Symptoms that deserve prompt medical attention include:
- severe abdominal pain
- pain that spreads to the back
- repeated vomiting
- signs of dehydration
- yellowing of the skin or eyes
- upper right abdominal pain, especially with fever or vomiting
- symptoms of low blood sugar, such as shakiness, sweating, confusion, or rapid heartbeat
- swelling of the face, lips, tongue, or throat
- trouble breathing
- a lump or swelling in the neck, hoarseness, or trouble swallowing
The point is not to expect these problems. The point is to know what not to ignore.
Mood, pleasure, and the psychology of eating
The psychological side of these medications deserves more attention.
Some patients feel emotionally better. They may experience less shame, less anxiety around food, and more confidence because cravings feel manageable for the first time in years.
Others feel strangely flat. They may lose interest in food, social meals, alcohol, or activities that previously brought pleasure. Some people feel unsettled by how quickly their appetite and body change.
Food is emotional for many people. When appetite is chemically reduced, that emotional system may need time to adjust.
Helpful questions to ask yourself:
- Do I feel calm around food or disconnected from food entirely?
- Am I eating enough, or am I avoiding food because appetite is gone?
- Am I becoming more flexible, or more fearful about eating?
- Is my mood improving, worsening, or flattening?
- Am I still enjoying social life, movement, and daily routines?
- Do I need support from a clinician, dietitian, or therapist?
If mood changes are significant, persistent, or include symptoms of depression or self-harm, seek medical help promptly.
A safer way to think about risk
A safer decision framework is not “Are these drugs good or bad?”
A better framework is:
- Benefit: What health problem am I trying to treat?
- Risk: What side effects or contraindications apply to me?
- Monitoring: Who is following my labs, symptoms, and progress?
- Lifestyle support: Am I protecting protein intake, muscle, hydration, and mental health?
- Sustainability: Can I afford and maintain this plan long enough for it to make sense?
- Exit plan: What happens if I stop, switch, or reduce the dose?
That kind of thinking keeps the decision grounded instead of emotional.
Mounjaro vs. Ozempic — Who Should Use Which
The honest answer is not “Mounjaro is better” or “Ozempic is safer.”
The honest answer is: it depends.
Both medications affect appetite, digestion, blood sugar, and weight. Both can cause side effects. Both require medical supervision. Both may be helpful for the right patient and inappropriate for another.
The decision should be based on your diagnosis, goals, medical history, risk profile, and access.
Efficacy is only one part of the decision
If the main question is average weight-loss effect, tirzepatide has generally shown greater average weight reduction than semaglutide in obesity-focused clinical research.
But average results do not decide individual care.
One person may lose more on semaglutide than expected. Another may tolerate tirzepatide poorly. Someone else may need a medication primarily for blood sugar control, while another person may be focused on chronic weight management.
Instead of asking, “Which one is strongest?” ask:
- Which one is approved for my specific use?
- Which one matches my medical history?
- Which one can I tolerate?
- Which one can I afford long-term?
- Which one does my clinician recommend and why?
Stronger is not always better if it is not sustainable.
Tolerability and dose escalation matter
Side effects often show up during the early weeks and after dose increases.
Some people tolerate semaglutide better. Others do better on tirzepatide. Some people cannot tolerate either at higher doses. Slower dose escalation may help, but that decision belongs with the prescribing clinician.
Questions worth discussing before starting:
- How often will my dose increase?
- What side effects should I expect?
- What symptoms should make me call you?
- Can we slow down dose increases if side effects are difficult?
- What should I eat around injection day?
- What should I do if I vomit or cannot stay hydrated?
Good prescribing is not just writing the prescription. It includes anticipating problems and having a plan.
Diabetes, cardiovascular risk, and medical history
For people with type 2 diabetes, both medications may help lower blood sugar, but the right choice depends on the full medical picture.
For someone with cardiovascular disease, kidney disease, a history of pancreatitis, gallbladder issues, diabetic eye disease, thyroid cancer risk, or multiple medications, the decision becomes more individualized.
Your clinician may consider:
- A1C and glucose patterns
- current diabetes medications
- hypoglycemia risk
- heart disease history
- kidney function
- digestive history
- gallbladder history
- pregnancy plans
- family history of medullary thyroid carcinoma
- previous response to GLP-1 medications
- insurance coverage and affordability
Some patients may also benefit from deeper assessment through metabolic testing and analysis, especially when weight, energy, metabolism, and nutrition planning need to be reviewed together.
Cost, access, and long-term planning
Cost is not a small detail. It is part of the medical decision.
These medications can be expensive without insurance, and coverage varies widely. Some plans cover them for type 2 diabetes but not for weight management. Some require prior authorization. Some patients qualify for savings programs, while others do not.
Before starting, ask:
- Is this covered under my diagnosis?
- What will my monthly cost be?
- Could coverage change?
- What happens if supply is interrupted?
- Can I sustain this for more than a few months?
- Is there a backup plan if I cannot continue?
A medication that works but cannot be sustained may create emotional and physical frustration if there is no long-term plan.
What neither drug replaces
Neither Mounjaro nor Ozempic replaces the foundations of care.
They do not replace:
- a protein strategy
- resistance training
- hydration
- sleep
- follow-up appointments
- side-effect monitoring
- behavior change
- mental health support
- long-term maintenance planning
They can make those habits easier to build for some people. But they do not build them for you.
A responsible plan treats medication as a tool inside a larger system.
Maryland Trim Clinic (MTC) in Laurel, MD
To avoid confusion, “MTC” here refers to Maryland Trim Clinic, not medullary thyroid carcinoma, which is a separate medical term mentioned in GLP-1 medication warnings.
Maryland Trim Clinic (MTC) in Laurel, MD can support people who are trying to make informed decisions about medical weight management, GLP-1 treatment, nutrition, body composition, and long-term maintenance.
How local medical support can help
A clinic setting can be helpful because these medications are not just about getting a prescription. Patients may need help deciding whether medication is appropriate, managing side effects, protecting muscle, setting realistic goals, reviewing progress, and planning for what happens if treatment changes.
For someone considering GLP-1 or GIP-based medication, MTC offers GLP-1 treatment options as part of its service list. Patients who need broader structure may also discuss a medical weight management program that supports weight-related goals with more than medication alone.
Some people also ask about non-surgical support after weight changes. In that context, non-invasive body contouring treatments may be discussed as an optional supportive service, not a replacement for nutrition, movement, medical monitoring, or long-term health habits.
If you are local to the area, Maryland Trim Clinic in Laurel, MD can be a starting point for a medically guided conversation about what fits your goals, health history, and current symptoms.
The Bottom Line
Mounjaro and Ozempic are genuinely significant medical tools.
They can improve blood sugar control. They can reduce appetite. They can help eligible patients lose weight when used appropriately. For many people, they create a level of relief around hunger and cravings that lifestyle changes alone never provided.
But they are not magic.
They come with side effects. They require monitoring. They may need to be continued long-term to maintain results. They can contribute to muscle loss if nutrition and strength training are ignored. They may affect digestion, mood, appetite, cost, and your relationship with food.
The people who tend to do best are not the ones who believe the hype or fear the worst. They are the ones who go in clear-eyed.
They understand that:
- side effects are real
- benefits can also be real
- medical supervision matters
- muscle preservation must be intentional
- stopping should be planned, not guessed
- cost and access are part of the decision
- medication works best inside a broader health strategy
That is the whole truth. Not the miracle version. Not the panic version. The useful version.
Medical disclaimer: This article is for educational purposes only and is not a substitute for medical advice, diagnosis, or treatment. Mounjaro, Ozempic, Zepbound, Wegovy, and related medications should only be used under the supervision of a qualified healthcare professional. Do not start, stop, or change any prescription medication without speaking with your prescriber.
Frequently Asked Questions
Q: What is the main difference between Mounjaro and Ozempic?
Ozempic is semaglutide, a GLP-1 receptor agonist. Mounjaro is tirzepatide, which activates both GLP-1 and GIP pathways.
In simple terms, both medications affect appetite, digestion, insulin response, and blood sugar regulation. Mounjaro works through two incretin hormone pathways, while Ozempic works primarily through GLP-1.
This difference may help explain why tirzepatide has generally shown greater average weight reduction in obesity-focused trials. But the better choice depends on the patient, diagnosis, medical history, side effects, cost, and clinician guidance.
Q: Will I regain weight if I stop taking these medications?
Many people regain weight after stopping GLP-1 or GIP-based medications, especially if no long-term maintenance plan is in place.
This is not a moral failure. These medications help manage biological signals related to appetite and fullness. When the medication is removed, hunger and food noise may return.
Before stopping, talk with your prescriber about:
- whether dose reduction is appropriate
- how often to monitor weight
- how to respond to early regain
- what nutrition structure should be in place
- how to maintain protein and resistance training
- what other treatment options may be appropriate
Do not stop suddenly without medical guidance, especially if you are using the medication for type 2 diabetes.
Q: Do Mounjaro and Ozempic cause muscle loss?
They can contribute to lean mass loss if weight loss is rapid and muscle-preserving habits are not in place.
Any major weight loss can include both fat and lean mass. The risk may be higher when appetite is very low, protein intake drops, and resistance training is absent.
To reduce the risk, prioritize:
- protein at each meal
- resistance training
- enough calories to function well
- hydration
- sleep
- gradual activity progression
- tracking strength and measurements, not just weight
A clinician or registered dietitian can help set protein goals that are appropriate for your body and medical history.
Q: Are there serious medical risks associated with these drugs?
Yes, although serious events are not the most common experience.
Potential risks include pancreatitis, gallbladder problems, severe gastrointestinal symptoms, dehydration-related kidney issues, low blood sugar when combined with certain diabetes medications, allergic reactions, and boxed warnings related to thyroid C-cell tumors based on animal data.
These medications are generally not recommended for people with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2.
Seek medical attention promptly for severe abdominal pain, repeated vomiting, trouble breathing, swelling of the face or throat, severe dehydration, or symptoms of low blood sugar.
Q: Which drug is better for someone with type 2 diabetes and heart disease?
That depends on the individual.
Semaglutide has established cardiovascular outcomes data in certain populations, while tirzepatide also has important metabolic effects and ongoing evidence development. But the best option for a person with type 2 diabetes and heart disease should be decided with a clinician who can review the full picture.
Important factors include:
- A1C level
- current diabetes medications
- hypoglycemia risk
- cardiovascular history
- kidney function
- weight goals
- side effect history
- insurance coverage
- contraindications
Do not choose based only on online weight-loss comparisons.
Q: How do these drugs affect appetite and cravings at a brain level?
These medications influence appetite signals in the brain as well as digestion and blood sugar regulation.
Many patients report that hunger feels quieter, cravings feel less urgent, and food becomes less mentally consuming. This is often described as reduced “food noise.”
That can be helpful, especially for people who have struggled with constant cravings or overeating. But it can also feel emotionally strange if food previously played a large role in comfort, celebration, social connection, or stress relief.
If appetite suppression becomes so strong that eating feels difficult or distressing, talk with your healthcare provider.
Q: How much do Mounjaro and Ozempic cost?
Costs vary widely based on insurance, diagnosis, pharmacy, location, manufacturer programs, and whether the medication is being prescribed for diabetes or weight management.
Without coverage, these medications can be expensive. With coverage, out-of-pocket costs may still vary significantly. Some plans cover diabetes indications but not weight-management indications.
Before starting, ask your prescriber, pharmacy, and insurance plan:
- Is this medication covered for my diagnosis?
- Do I need prior authorization?
- What will my monthly out-of-pocket cost be?
- Are there savings programs I qualify for?
- What happens if coverage changes?
- Is there a long-term affordability plan?
Cost should be discussed before treatment begins, not after the medication starts working.
When to Consider Professional Support
Some people benefit from structured medical guidance when deciding whether a GLP-1 medication fits their health history, weight goals, side-effect concerns, and long-term maintenance plan. If you are in Maryland and want a careful, medically guided conversation, Maryland Trim Clinic can help you explore your options without treating medication as a one-size-fits-all solution.