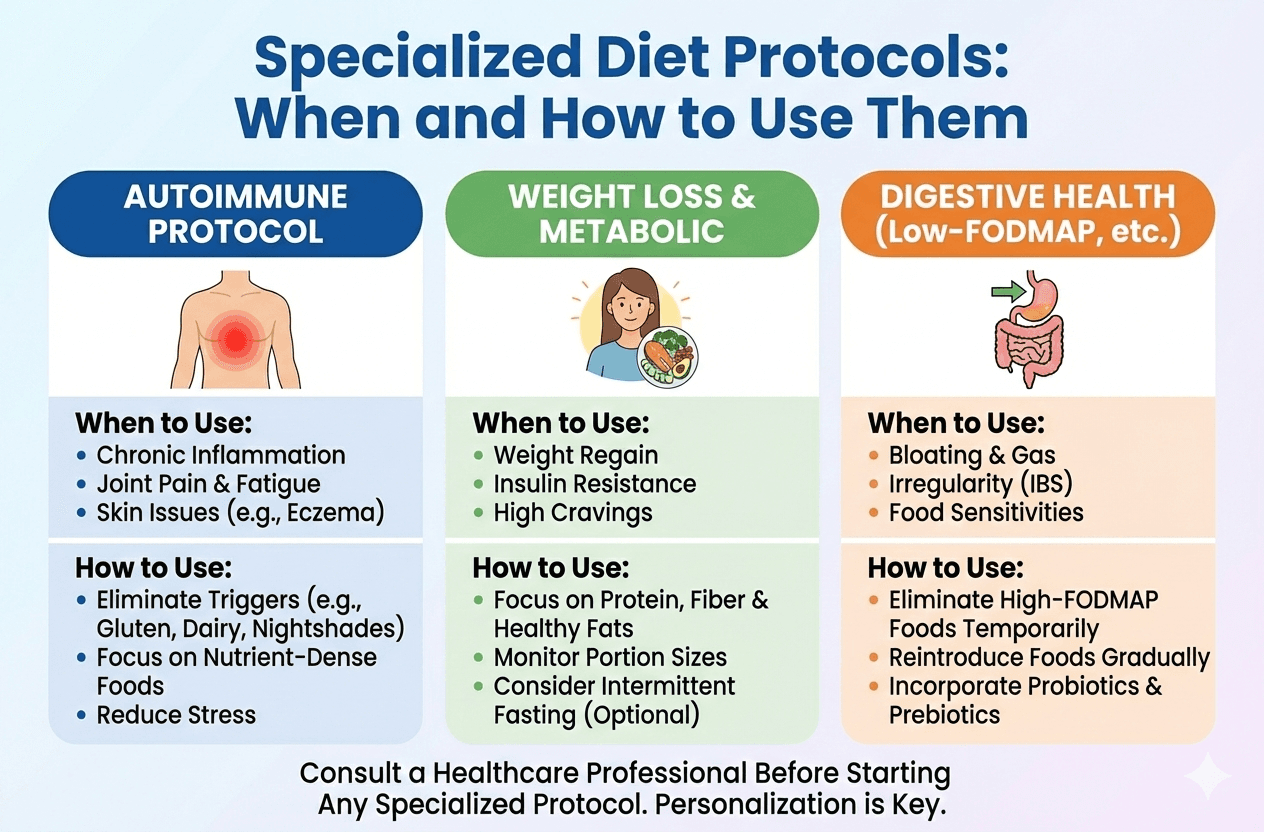
Specialized Diet Protocols: When and How to Use Them

Carnivore, keto, elimination, here is when they actually work.
Whether you are a nutrition professional guiding clients, or someone personally exploring dietary changes, you have likely encountered dramatic transformation stories. You've seen influencers tout ketogenic protocols or heard friends swear by complex elimination approaches. The question isn't whether these specialized diets can work, it is determining who actually benefits from them versus those who would thrive on a more balanced, inclusive approach.
This clinical decision sits at the heart of effective nutritional care. Recommend a restrictive protocol too quickly, and you risk creating unnecessary food fear, social isolation, or disordered eating patterns. Wait too long to suggest a therapeutic intervention, and a person might continue suffering with symptoms that could be directly addressed through targeted dietary changes.
Let's break down the framework for making these decisions with confidence, utilizing nutritional counseling and coaching principles that prioritize long-term wellbeing.
Act 1: Client Profiles That Benefit from Specialized Protocols
Not every symptom requires a drastic dietary overhaul. However, certain physiological profiles respond exceptionally well to targeted nutritional therapies.
Autoimmune Conditions and Inflammatory Responses
Individuals with diagnosed autoimmune conditions, such as rheumatoid arthritis, Hashimoto's thyroiditis, psoriasis, or inflammatory bowel disease, often benefit from elimination protocols. The Autoimmune Protocol (AIP), a phased elimination diet removing common inflammatory triggers, has shown clinical promise in reducing disease activity.
The mechanism is straightforward: certain foods may trigger immune responses in susceptible individuals. By temporarily removing potential triggers and systematically reintroducing them, you can identify specific problematic foods rather than imposing permanent, lifelong restrictions.
Key indicators for an autoimmune protocol:
- Diagnosed autoimmune condition with active, disruptive symptoms.
- Elevated inflammatory markers on bloodwork (e.g., CRP, ESR).
- Poor or incomplete response to standard medical treatment alone.
- Willingness to commit to a strict 6-to-8 week protocol.
- Stable mental health without a history of restrictive eating disorders.
Metabolic Dysfunction
Ketogenic and low-carbohydrate approaches shine for individuals experiencing metabolic dysfunction. Those dealing with insulin resistance, prediabetes, type 2 diabetes, or Polycystic Ovary Syndrome (PCOS) often experience dramatic improvements in glycemic control, insulin sensitivity, and hormonal balance. To understand more about how insulin resistance develops, you can review resources from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK).
The metabolic switch from glucose to ketone utilization can effectively "reset" insulin signaling pathways. For someone who has been on a blood sugar roller coaster for years, the resulting stable energy and reduced cravings can be life-changing.
Key indicators for metabolic protocols:
- Fasting glucose >100 mg/dL or HbA1c >5.7%.
- A diagnosis of PCOS accompanied by insulin resistance.
- Significant visceral adiposity (belly fat) alongside poor metabolic markers.
- A clear history of carbohydrate-driven energy crashes.
- Medical clearance from a primary care physician (especially if currently taking diabetes medications).
Digestive Disorders
Individuals suffering from Irritable Bowel Syndrome (IBS), Small Intestinal Bacterial Overgrowth (SIBO), or suspected food sensitivities are prime candidates for structured elimination protocols. The low-FODMAP diet, the Specific Carbohydrate Diet (SCD), or broader elimination approaches can help identify the exact dietary triggers driving digestive distress.
Unlike autoimmune or metabolic applications, digestive protocols often require highly nuanced customization. A food that triggers severe symptoms in one IBS patient might be perfectly tolerated by another. For more context on managing IBS, the NIDDK provides comprehensive guidelines on the condition.
Key indicators for digestive protocols:
- Chronic digestive symptoms despite trying basic interventions (like increasing water or general fiber).
- Positive SIBO breath test or strong clinical suspicion from a doctor.
- A predictable pattern of symptoms occurring shortly after meals.
- Failed responses to standard probiotics, stress management, or general healthy eating.
- Clearance from a gastroenterologist to rule out serious pathology (like celiac disease or colon cancer).
Neurological Applications
The ketogenic diet has a long-established efficacy for epilepsy management. Furthermore, emerging neurological research suggests potential benefits for migraine prevention, managing certain neurodegenerative conditions, and supporting traumatic brain injury recovery.
These applications are highly specialized and typically require strict medical supervision alongside precise macronutrient tracking. In these cases, nutritional support serves to implement a doctor's medically-prescribed protocol rather than initiating it independently.
Key indicators for neurological protocols:
- Direct recommendation or prescription from a neurologist.
- Refractory epilepsy or frequent, debilitating migraines.
- The capacity for precise, daily macronutrient tracking and adherence.
- Strong, ongoing coordination with a medical care team.
When NOT to Use Elimination Protocols
Recognizing contraindications is just as important as identifying appropriate candidates. Restrictive diets can do more harm than good in the wrong circumstances.
Red flags that indicate specialized protocols should be avoided:
- An active eating disorder or a documented history of restrictive eating patterns.
- A poor relationship with food, characterized by significant food anxiety or guilt.
- Unrealistic or rapid weight loss expectations acting as the primary motivation.
- An inability to commit to the proper timeline (e.g., trying to rush the reintroduction phase).
- Pregnancy or breastfeeding (in the vast majority of cases, energy demands are too high for restriction).
- Adolescents, unless under strict, specialized medical supervision.
- Individuals seeking "quick fixes" rather than sustainable, long-term health solutions.
For these profiles, a balanced, inclusive approach focusing on adding nutrient density, improving meal timing, and building a positive psychological relationship with food serves them far better than restriction.
Act 2: Practical Implementation and Meal Planning Systems
Pre-Protocol Assessment
Before launching into any specialized dietary protocol, it is vital to establish comprehensive baselines. This baseline data becomes the compass for evaluating whether the protocol is actually working.
Objective measures to gather:
- Relevant lab work (comprehensive metabolic panel, thyroid cascade, inflammation markers).
- Weight, body composition, and relevant circumferences.
- Blood pressure and resting heart rate.
- Baseline photos (if appropriate and comfortable).
Subjective tracking measures:
- Symptom severity scales (rating pain, fatigue, or digestive issues on a 0-10 scale).
- Sleep quality logs.
- Daily energy level tracking.
- Mood and mental clarity assessments.
- A current, honest 3-day typical diet recall.
The Phased Elimination Approach
Most therapeutic protocols fail because they are treated as permanent lifestyles rather than temporary diagnostic tools. They work best when implemented in structured phases:
Phase 1: Elimination (3 to 8 weeks) Remove identified trigger categories completely.
- For Autoimmune protocols: Typically excludes grains, legumes, dairy, eggs, nightshades, nuts, seeds, and certain food additives.
- For Ketogenic approaches: Carbohydrates drop drastically to 20-50g daily.
- For FODMAP elimination: High-FODMAP foods are removed across all categories.
The elimination phase should be long enough to observe meaningful physiological changes, but not so extended that nutritional deficiencies or psychological strain develop.
Phase 2: Reintroduction (4 to 12 weeks) Systematically reintroduce eliminated foods one at a time, typically in 3-day trials. This phase requires meticulous tracking. A standard reintroduction cadence looks like this:
- Day 1: Small serving of the test food.
- Day 2: Moderate serving if no initial reaction occurs.
- Day 3: Full serving if completely tolerated.
- Days 4-6: Return to the strict elimination baseline, monitoring carefully for delayed reactions.
Document any symptoms during this phase: digestive changes, energy shifts, skin reactions, joint pain, mood swings, or sleep disruption.
Phase 3: Personalization (Ongoing) Based entirely on the reintroduction results, create a personalized, long-term eating template. This template includes all safely tolerated foods and strategically limits or completely excludes the confirmed triggers.
Meal Planning Templates
Providing a structured template reduces decision fatigue during the challenging initial phases of a new diet. Here are structural examples of how to build meals for different protocols.
Autoimmune Protocol (AIP) Sample Structure:
- Breakfast: Sweet potato hash with ground meat, sautéed greens, and avocado.
- Lunch: A large salad with grilled chicken, roasted vegetables, and a simple olive oil and lemon dressing.
- Dinner: Grass-fed beef with roasted root vegetables and a side of probiotic sauerkraut.
- Snacks: Bone broth, fresh fruit, plain coconut yogurt, or baked plantain chips.
Ketogenic Sample Structure:
- Breakfast: Eggs cooked in butter, served with bacon and half an avocado.
- Lunch: Wild salmon salad mixed with olive oil mayo, served over mixed dark greens.
- Dinner: Ribeye steak topped with butter-sautéed mushrooms alongside asparagus.
- Snacks: Macadamia nuts, hard cheese, olives, or homemade fat bombs.
Low-FODMAP Sample Structure:
- Breakfast: Oatmeal prepared with lactose-free milk, topped with blueberries and walnuts.
- Lunch: Grilled chicken breast with a side of quinoa, cooked carrots, and green beans.
- Dinner: Baked white cod alongside roasted zucchini and potatoes.
- Snacks: Plain rice cakes with peanut butter, a handful of grapes, or hard cheese.
Client Education and Expectation Setting
Transparency prevents premature protocol abandonment. Ensure these expectations are clear before day one:
- The Timeline: Explain that feeling worse before feeling better is common. The first 3-7 days often involve "carb withdrawal," changes in digestion, or fatigue. Real assessment usually begins at week three.
- Social Navigation: Provide actionable scripts for declining foods at gatherings, strategies for ordering at restaurants, and ways to communicate dietary boundaries politely without needing lengthy explanations.
- The Temporary Nature: Reinforce that this is a diagnostic tool, not a permanent lifestyle. The goal is gathering data about how the body responds.
- Realistic Outcomes: Define success metrics that go beyond the scale—focus on symptom reduction, energy improvement, and lab marker changes.
Supplement Considerations
Because elimination protocols are restrictive by nature, they carry a real risk of nutrient gaps.
- AIP Concerns: Missing dairy and nuts can lead to low Calcium and Vitamin E. Consider high-quality calcium citrate and mixed tocopherols.
- Ketogenic Concerns: The rapid loss of water weight flushes out essential minerals. Electrolytes (sodium, potassium, magnesium) and fiber are critical. Consider electrolyte supplementation, psyllium husk, and magnesium glycinate.
- Low-FODMAP Concerns: Removing diverse carbohydrates starves beneficial gut bacteria, reducing prebiotic fiber. Consider specific low-FODMAP probiotic strains and the very gradual reintroduction of tolerated prebiotics.
Always work within a defined scope of practice and coordinate with a medical team for any therapeutic dosing.
Act 3: Monitoring and Adjusting Therapeutic Diets
Biomarkers to Track
Subjective feelings are important, but objective data is vital. Schedule lab reassessments at strategic intervals. If you need professional assistance tracking these metrics, utilizing comprehensive metabolic testing and analysis can provide invaluable insights into how a diet is affecting your body on a cellular level.
At 4 to 6 weeks:
- Metabolic protocols: Check fasting glucose, fasting insulin, HbA1c, and a lipid panel.
- Inflammatory protocols: Check CRP and ESR.
- General safety: Run a CBC and CMP to ensure no adverse effects are developing.
At 3 to 6 months:
- Comprehensive metabolic panel.
- Complete thyroid function panel (TSH, free T3, free T4).
- Vitamin D, B12, and iron studies (especially if the protocol limits these nutrients).
- Body composition reassessment.
Note: Improving symptoms without improving biomarkers may indicate a placebo effect or that you're tracking the wrong markers entirely. Conversely, improving biomarkers without symptom relief suggests the symptoms have a different root cause.
Symptom Journals and Subjective Measures
Daily tracking during the elimination and reintroduction phases should capture a holistic view of well-being:
- Bowel movements (tracking frequency and consistency via the Bristol stool scale).
- Energy levels (rated on a 1-10 scale, noted in both the morning and afternoon).
- Sleep quality (total hours and a restfulness rating).
- Mood and perceived mental clarity.
- Pain levels (if relevant to the condition).
- Specific symptoms being targeted by the protocol.
Digital apps can streamline this process, but a simple notebook or spreadsheet works equally well. Consistency is the only mandatory requirement.
Reintroduction Protocols
The reintroduction phase provides the most valuable diagnostic information, yet it is the phase most often rushed or skipped entirely. A structured sequence is non-negotiable.
For the Autoimmune Protocol (AIP): Reintroduce foods starting with the most commonly tolerated, moving toward the least tolerated:
Egg yolks
Seed-based spices
Nut-based spices
Seed and nut oils
Egg whites
Nightshade spices
Nightshade fruits and vegetables
Alcohol (in very small quantities)
Legumes with edible pods (like green beans)
All other legumes
Grass-fed dairy
Conventional dairy
Gluten-free grains
Gluten-containing grains
For the Low-FODMAP Diet: Reintroduce by FODMAP category (fructans, GOS, lactose, polyols, fructose) rather than broad food groups. Test high-FODMAP foods carefully within each specific category.
For Ketogenic Diets: If transitioning out of ketosis, do not jump straight to high-carb meals. Gradually increase carbohydrates by 5-10g daily, carefully monitoring glycemic control and watching for the return of previous symptoms.
When to Transition Back to Balanced Eating
Successful therapeutic protocols should eventually transition to sustainable, everyday patterns.
Signs it is time to expand the diet:
- You have identified specific triggers and created a sustainable, personalized exclusion list.
- Primary symptoms have resolved or significantly improved.
- Lab markers have normalized.
- There is noticeable social or psychological strain from the restriction.
- Nutritional concerns or deficiencies are beginning to emerge.
- You have collected 3 to 6 months of solid data.
Signs to continue the current protocol:
- Symptoms are still actively improving day-to-day.
- Quality of life is reported as high without psychological distress.
- Medical supervision strongly recommends continuation (e.g., for epilepsy).
- There is a clear, undeniable symptom return during any reintroduction attempts.
Long-Term Sustainability Considerations
Very few individuals should remain on strict elimination protocols indefinitely.
- Ketogenic: Some individuals with epilepsy, severe metabolic conditions, or neurodegenerative diseases may benefit from long-term ketogenic eating. However, most people do better cycling into a moderate, low-carb approach once their metabolic flexibility improves.
- AIP/Elimination: The end goal is always personalization, a unique template based on identified triggers. Most people find they can comfortably tolerate 70-90% of initially eliminated foods after a proper, slow reintroduction.
- Low-FODMAP: This is explicitly a short-term diagnostic protocol. Long-term restriction of FODMAPs actually damages gut microbiome diversity by starving healthy bacteria. The ultimate outcome should be finding a personalized portion threshold for each FODMAP category, not avoiding them forever.
Exit Strategies
Sometimes, a protocol simply isn't working. Knowing when to pivot is crucial.
- No improvement by week 6 to 8: Reassess whether this is the right physiological approach, or if other root causes (like chronic stress or underlying infections) need investigation.
- Worsening symptoms: Some protocols exacerbate certain conditions. For example, carnivore diets may worsen existing, undiagnosed kidney issues; very low-carb approaches might impair thyroid function in highly susceptible individuals.
- Psychological distress: If food anxiety, social isolation, or restrictive eating patterns begin outweighing physical benefits, immediate protocol modification is required.
- Poor adherence: If maintaining 85%+ compliance is impossible, the protocol simply does not fit the lifestyle or current capacity. Consider less restrictive, step-down alternatives.
Having a clear exit strategy discussed before starting prevents anyone from feeling like a "failure" if the protocol isn't the right biological fit.
The Decision Framework
Before recommending or starting any specialized dietary protocol, run through this final checklist:
- Medical necessity: Is there a officially diagnosed condition or a clear, documented symptom pattern that warrants a strict therapeutic intervention?
- Failed conventional approaches: Has a balanced, inclusive, nutrient-dense approach been properly attempted first?
- Psychological readiness: Is there sufficient mental and emotional capacity to handle temporary restriction without triggering food anxiety?
- Logistical capacity: Is there time and energy to handle the extensive meal planning, food preparation, and social navigation required?
- Medical clearance: Has there been communication and coordination with a primary healthcare team?
- Baseline data: Are objective labs and subjective symptom measures recorded to evaluate future outcomes?
- Clear protocol: Are the elimination, reintroduction, and personalization phases distinctly outlined?
- Defined success metrics: What specific, measurable improvements constitute "success"?
- Exit strategy: What exactly happens if the protocol doesn't work or causes adverse problems?
If you cannot confidently check most of these boxes, jumping into a specialized protocol is likely premature.
Maryland Trim Clinic (MTC) in Laurel, MD
Navigating specialized diets, managing metabolic health, and achieving sustainable weight loss can be overwhelming to tackle alone. Having a structured, medically supervised environment ensures you are using the right protocols safely. Located in Laurel, MD, the Maryland Trim Clinic (MTC) provides evidence-based care tailored to your unique biology.
Whether you need guidance transitioning into a specialized diet for metabolic health, or you are looking for a comprehensive medical weight loss program to address the root causes of weight regain, our team is equipped to support you. We believe in moving away from crash diets and focusing instead on sustainable, personalized solutions that fit your life. If you are struggling to find an approach that works for your body, visit the Maryland Trim Clinic online to explore how our clinical expertise can support your health journey.
Disclaimer: The information provided in this article is for educational purposes only and is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or a qualified healthcare provider before beginning any new diet, especially if you have pre-existing health conditions or are taking medication.
Frequently Asked Questions
Q: How long should an elimination diet last? A: The elimination phase typically lasts 3 to 8 weeks, heavily depending on the specific condition being addressed. Autoimmune protocols often require 6-8 weeks for systemic inflammation to settle, while FODMAP elimination is usually 2-6 weeks. The reintroduction phase adds another 4-12 weeks. Total protocol duration is usually 8-16 weeks before arriving at a personalized long-term template. Extending elimination phases longer than this risks nutritional deficiencies and unnecessary psychological strain.
Q: Can I exercise normally on keto or carnivore diets? A: Exercise capacity typically decreases during the first 2-4 weeks of ketogenic or carnivore protocols as the body adapts from using glucose to using fat for fuel. High-intensity performance may remain compromised initially. However, once "keto-adapted" (usually after 4-8 weeks), most individuals maintain endurance exercise very well, and strength training is generally well-tolerated. Proper electrolyte supplementation is absolutely crucial for exercise performance on these protocols.
Q: What is the difference between an elimination diet and a restrictive diet? A: Elimination diets are time-limited diagnostic tools with a highly structured reintroduction phase designed to identify specific physiological triggers. The end goal is personalization, not permanent restriction. Restrictive diets, on the other hand, involve the ongoing, indefinite limitation of foods or food groups, often driven by weight loss goals or rigid food rules. If a "temporary" elimination diet extends beyond 4-6 months without a proper reintroduction testing phase, it has morphed into a restrictive diet.
Q: How do you prevent nutrient deficiencies on specialized protocols? A: Prevention starts with a pre-protocol assessment of your baseline nutritional status through lab work (checking vitamin D, B12, iron, etc.). During the protocol, you must heavily emphasize nutrient density within the allowed foods, eating colorful vegetables within guidelines and ensuring variety. Strategic, targeted supplementation can address known gaps (like calcium on AIP or electrolytes on keto). Most importantly, keeping the elimination phase strictly time-limited is the best defense against deficiencies.
Q: When should I seek a medical professional rather than trying a protocol myself? A: You should always coordinate with a medical professional if you have diagnosed medical conditions, take daily medications (especially for diabetes, blood pressure, or thyroid function), or exhibit red flag symptoms like unexplained weight loss or severe pain. Active eating disorders, pregnancy, breastfeeding, and complex medical histories require direct medical supervision. Never attempt a therapeutic ketogenic diet for a condition like epilepsy without a neurologist's explicit guidance.
Ready to Find the Right Nutritional Protocol for Your Body?
Stop guessing and start healing. Contact Maryland Trim Clinic today to schedule a consultation, and let our medical team help you build a personalized, sustainable nutritional strategy that addresses your unique health needs.